

SICK DAY
Cannabis Is Coming for Big OTC Cold + Flu

Over the past decade, we’ve seen that cannabis has a unique way of biting the ankles of giants. While we frequently discuss how it’s stealing share from opioids and alcohol, we rarely focus on the everyday medicine cabinet. And by extension, how cannabis could eat into the massive $400BN “self-care” OTC market.1
Today’s SUNDAY SESH focuses on one category sitting directly in cannabis’ crosshairs—the $35BN U.S. cold and flu market.2 And it’s not hard to see why: endless pharmacy aisles filled with ancient syrups, pills, sprays, nutraceuticals, and homeopathic remedies that promise many things but mostly do none as your body does the real work.
That matters—especially as cannabis sheds its 100+ year archaic stigma. Whether it’s HHS’ groundbreaking analysis under Biden, Trump’s push to reschedule, or the decades of independent medical research, the conclusion is clear:
Cannabis is real medicine.
For 55+ years, cannabis as a Schedule I drug meant the government claimed it had no accepted medical use. Somehow they ignored thousands of years of documented history, including in our own country. More importantly, they ignored the countless stories from pop culture and people just like me who spent decades watching real people find real relief.
Even for the common cold and flu.
When it comes to cannabis, SUNDAY SESH tries to bridge Wall Street and Main Street: how the industry will evolve, and how real-world experiences can change minds and standards of care. Combined, we paint a vision for the future.
So let’s pull out the terpy RSO, maybe pour a hot cup of cannabis-infused tea, and dive deep on another hill we’ll die on: cannabis is coming for OTC cold and flu. And it’s my bet Big CPG is asleep at the wheel after one too many doses of NyQuil.
Welcome to SUNDAY SESH.

2/WHAT IS THE COMMON COLD?
Before we dive into the thesis, a quick disclaimer: I am not a doctor, and these are not recommendations. But I do have reps: I was one of the 1-in-15 kids who needed tympanostomy tubes, not once but twice before age 10. My son also needed tubes—not once but also twice before age 10. So let’s just say I know my way around the ENT medical complex.
The common cold is exactly what it sounds like: common. It’s a viral infection of the upper respiratory tract, usually centered around the nose, throat, and sinuses. Symptoms are familiar: runny nose, congestion, sneezing, sore throat, cough, watery eyes, headache, low-grade fever, and that general “I feel like shit” malaise made worse by terrible nights of sleep.
The flu is different, but the experience rhymes. Influenza is also a viral respiratory illness, but it usually hits harder and faster. Putting aside Rx antivirals like Tamiflu, the consumer playbook is still mostly symptom management. And OTC meds are virtually identical to what you'd reach for with a cold. Same molecules, different box.
When you get these bugs, the virus isn’t “stuffing” your nose with mucus. Instead, infected respiratory cells release inflammatory mediators, including cytokines and chemokines, which call immune cells into the area and turn up local inflammation. This inflammatory cocktail is the source of the misery.
To state the obvious, what we reach for in the medicine cabinet is not curing the underlying virus. It helps alleviate symptoms as the virus naturally runs its course.
Even the claims of relief are spurious. Recently, the FDA unanimously concluded as much—finding no efficacy for oral phenylephrine, a main active ingredient found in over 250 OTC cold meds like Sudafed PE, DayQuil Severe, NyQuil Severe, and Tylenol Sinus.
This is critical to digest.
3/BUYER BEWARE
Regardless of questionable benefits, consumer feedback on OTC cold meds is universal: either you feel like a zombie or you feel wired. And therefore, you can’t stay awake or you can’t sleep.
For me, this “ping-ponging” was all too familiar growing up. As a kid, I vividly remember turning into a fucking werewolf after taking these drugs before bed. I couldn’t sleep, which left me feeling worse the next day. We’ve all been there.
To avoid that, today tens of millions of adults reach for drugs like NyQuil—a potent cocktail that includes Doxylamine (antihistamine) and ethyl alcohol (booze). This product basically puts you the fuck down, leaving many groggy. Why? Because doxylamine has a long half-life of ~10-12 hours. Not to mention, many products are still loaded with Blue No. 1 and Red No. 40 food dyes. (Hey Big CPG: wake up, you sell medicine in 2026.)
Still, these OTC drugs carry meaningful risks. Many products are “stacked” with multiple active ingredients, where patients can misdose or unknowingly combine drugs that interact with prescriptions. In addition, regulators have spent decades playing an endless game of “whack-a-mole” to ensure CVS isn’t pushing meth disguised as a cold remedy.
Anyone remember Sudafed’s “Medicine Head” commercials from the late ‘90s that promised alertness?
If you don’t, the upshot was that Sudafed contained pseudoephedrine, which later became tightly controlled because it’s a precursor to methamphetamine.
Lovely. No wonder I couldn’t sleep.
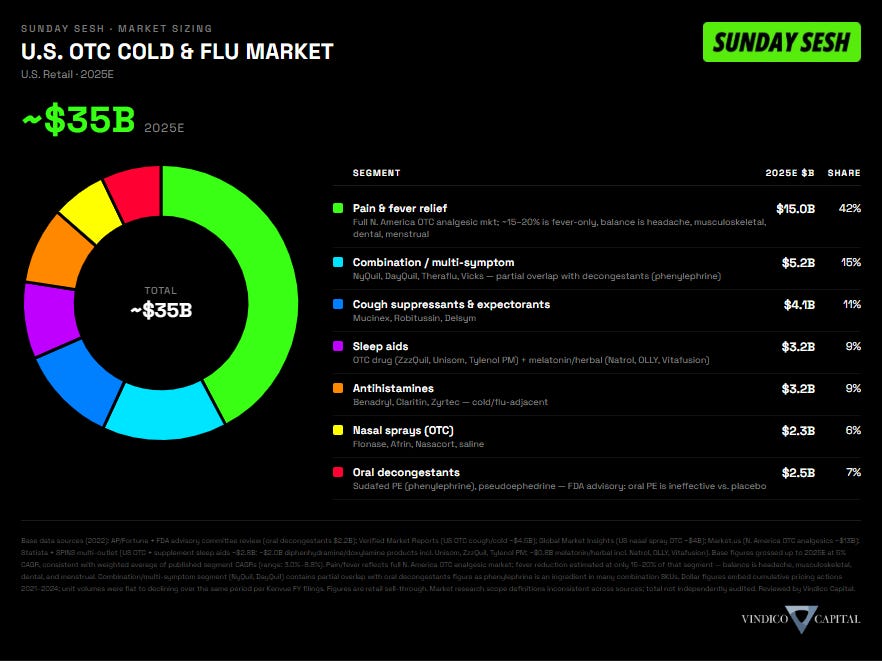
4/LET’S SIZE THIS MARKET
The addressable market is massive because "cold and flu" is not one category. It is a bundle of overlapping symptoms: cough suppressants and expectorants, antihistamines, decongestants, nasal sprays, and multi-symptom combinations (like NyQuil). Plus, it includes close adjacencies—like pain, fever relief and sleep—that customers often reach for when they get these bugs.
These drugs are the top two reasons why consumers still go to drug stores. Next time you walk into a CVS or Walmart, check out how much real estate the cold, flu and pain aisles cover. It’s massive.
Takeaway? This is a giant $35BN U.S. market.
5/ ECS UNLOCKS REAL SCIENCE
The cannabis-for-colds argument is not just “I took a gummy and felt better.” That may be where the idea starts, but the better question is why it might work at all. Beyond the sedation use-case to get better sleep—one of the main reasons why medical patients turn to cannabis—the biology runs deeper.
The answer likely lives inside inflammation, immune signaling, and the endocannabinoid system (“ECS”). We’ve discussed this in a prior SESH.
Early research is promising. Studies suggest cannabinoids may interact with inflammatory signaling pathways that are relevant to cold and flu symptoms. CB2 receptors, which are concentrated in immune-related tissues and cells, appear to help modulate the immune response. Not by turning inflammation off, but by acting more like a brake when the response becomes excessive.
A 2021 systematic review found cannabinoids—especially CBD, CBG, and CBD+THC combinations—often reduced inflammatory cytokines in animal models, while THC alone was less consistent. A separate lung-cell study found CBD-rich cannabis extracts reduced IL-6 and IL-8, two cytokines tied to airway inflammation and immune response.
On the antiviral side, the research is earlier and less proven but still relevant. A 2023 review summarized antiviral signals from hemp cannabinoids around viral entry, replication, and immune response. And CBD showed enough mechanistic activity to be tested in mild/moderate COVID, though the randomized trial did not show a clean benefit.
So the honest read: the biology is real, but the clinical bridge is unfinished. Schedule III classification should help close that gap. I’ll drop some relevant existing research in the comments to show what’s already been done.
Call it a hunch, but I’m wildly optimistic.
6/ WEED UNLOCKS BRO SCIENCE
“It’s good for the flu.” — “Legalize It” // Peter Tosh (1976)
Every great cannabis use-case typically gets exposed by “bro science” influenced by pop culture. And consumers don’t wait for white papers when they feel like shit. Peter Tosh, Bob Marley, Willie Nelson, Dr. Dre, and Cypress Hill carried the message through music. And movies like Caddyshack, Friday, Dazed and Confused, Half Baked, and Dallas Buyers Club only reinforced it.
That’s always been the cannabis playbook. The culture finds the use-case first. Science shows up later. Regulators show up last.
If we step back, OTC cold + flu meds really come down to two distinct use cases:
Reduce symptoms, which as noted is often spurious; and
Aid sedation to force you to ignore them.
That creates two very interesting seams: daytime symptom relief, and sleep.
The sleep angle should be obvious. I’ve previously discussed that global consumers have already figured out cannabis—like popping a gummy—can be more efficacious, and potentially safer, than popping an Ambien (Rx / zolpidem) or a Unisom (OTC / doxylamine succinate). And for millions it’s not even a debate anymore. Edibles across regulated and hemp exceed $8-12BN just in the U.S.
The $5BN OTC multi-symptom market—like NyQuil—already sells sleep. So if cannabis is already nipping at sleep aids when you’re not sick, nighttime cold meds are an obvious next bite. Especially since gummies cost ~$1.25-$2.00 per serving, which is on par with OTC alternatives.
The daytime side—relieving symptoms while you’re awake—is also where I’m optimistic. But I recognize the potential controversy given cannabis’ main cannabinoid—THC—is “intoxicating.”
On one hand, we’re forced to work through colds while dealing with “medicine head.” And millions of Americans already consume medical cannabis during the day. On the other hand, no one wants to show up stoned to a Board meeting. Including me. Cannabis and daytime don’t work for my lifestyle, ever.
So this is where I think the future gets interesting: micro-doses of THC (or none at all), complemented by more aggressive dosing of non-intoxicating cannabinoids like CBD and CBG. These minors may knock the funk out of the cold without knocking you out of your day.
And if you’re just too sick to work, then all bets are off. At that point, you just want relief—something that calms the body, helps you rest, and maybe lets you doze off during the day.
The point is simple: the market already exists. Consumers just might not realize cannabis belongs in the conversation. Folks like me—who’ve been relying on cannabis for decades to battle these bugs—will help light the path.
Think of the DayQuil || NyQuil combo. But made with cannabinoids.
7/FIN: CANNABIS IS A PERFORMANCE TOOL
True to form, I eat my own cooking. I’ll keep my personal routine high-level because this isn’t medical advice, and everyone’s body reacts differently. But when I’m sick and reaching for cannabis, I generally care about four things: quality, full-spectrum effects, form factor, and strain—in that order. Whether I’m trying to sleep or function.
My preferences have been further refined as the “green wave” spread. More access to more products from world-class teams has let me dial in my own standards of care across multiple major and minor cannabinoids, many of which are non-intoxicating. If you’re interested, I’ll drop the full “when I’m sick” stack in the chat— what I use, when I use it, what I avoid, and why.
To conclude, the status quo OTC cold and flu market is ripe for change. Existing products are ancient, potentially dangerous, and provide a mediocre experience at best. Even the FDA has started saying the quiet part out loud: most of this stuff doesn’t work.
Cannabis might not be the panacea, but neither is NyQuil or Robitussin. And that is the entire point—cannabis is simply a performance tool.
In 2026, it’s crazy to me that no one in the industry has leaned hard into this category. Very few even talk about it.
Perhaps that will be you. Ping me, I might be able to help.
Onward,
SUNDAY SESH

Perrigo 2025 Investor Day presentation, citing Nicholas Hall.
U.S. OTC retail, 2025E. “Cold & flu” defined as the full sick-day OTC basket: pain & fever relief, combination/multi-symptom cold meds, cough suppressants & expectorants, sleep aids, antihistamines, nasal sprays, and oral decongestants. Figures grossed up from 2022 base data at 5% CAGR. See chart for segment breakdown and sourcing.
***Disclaimer: Not financial or investment advice, do your own work; this is intended for sophisticated investors. No conflicts, no MNPI, these are my own opinions, and no representation that what’s presented is accurate. As disclosed, authors of SUNDAY SESH hold common shares and derivatives of companies mentioned and they have no obligation to update or disclose changes. No representation is made as to accuracy or completeness. Past performance is not indicative of future results. And as always, cannabis was used frequently in the authorship to creatively solve problems. Know what you own.
Excellent! Would very much be interested in your findings/protocol. Cheers, J
What the Research Actually Says
The evidence does not say cannabis cures colds or the flu. The more honest read is that cannabinoids interact with immune and inflammatory pathways that overlap with why viral illnesses feel so miserable: cytokines, airway inflammation, congestion, pain, sleep disruption, and systemic inflammation.
Cannabis Use and Systemic Inflammation — CARDIA Study
Year Published: 2019
Possible Indication: Systemic inflammation; cytokine response; biomarker signal
Key Takeaway: Human observational study looking at inflammatory markers including CRP, fibrinogen, and IL-6. Some markers appeared lower in cannabis users, but the association weakened after adjustment. Useful evidence of a possible signal, not proof.
Link: https://pmc.ncbi.nlm.nih.gov/articles/PMC6883146/
Cannabis Use and Inflammatory Biomarkers
Year Published: 2020
Possible Indication: Systemic inflammation; cytokine response; mixed/negative biomarker signal
Key Takeaway: Another human biomarker study found cannabis use was not clearly associated with lower hs-CRP, IL-6, or fibrinogen. This is an important counterweight to the more bullish inflammation narrative.
Link: https://pmc.ncbi.nlm.nih.gov/articles/PMC7894624/
Cannabinoids and Inflammatory Cytokines — Systematic Review
Year Published: 2021
Possible Indication: Cytokine response; inflammation; immune modulation
Key Takeaway: Broad review of in vivo studies found cannabinoids, especially CBD, CBG, and CBD+THC, often reduced inflammatory cytokines. This is one of the best citations for the cytokine-modulation thesis, although much of the evidence is preclinical rather than human clinical.
Link: https://pmc.ncbi.nlm.nih.gov/articles/PMC8266561/
CBD-Rich Cannabis Fraction and Lung Inflammation Markers
Year Published: 2021
Possible Indication: Respiratory inflammation; cytokine response; cold/flu research rationale
Key Takeaway: In lung-cell models, a CBD-rich cannabis extract reduced inflammatory markers including IL-6 and IL-8. Relevant to respiratory inflammation, but still cell-line/preclinical evidence, not proof that cannabis treats colds or flu.
Link: https://www.nature.com/articles/s41598-021-81049-2
CBD and Mild/Moderate COVID-19 — Randomized, Double-Blind Placebo-Controlled Trial
Year Published: 2022
Possible Indication: Viral illness; antiviral; cytokine response; negative/neutral efficacy signal
Key Takeaway: One of the more direct viral-illness tests. CBD 300 mg/day added to standard care did not show convincing clinical benefit in COVID progression. Important negative/neutral clinical evidence.
Link: https://pmc.ncbi.nlm.nih.gov/articles/PMC9587798/
Cannabis Use and Sinonasal Symptoms — U.S. Adult Study
Year Published: 2022
Possible Indication: Cold symptoms; nasal congestion; sinus symptoms
Key Takeaway: Regular cannabis users reported lower odds of sinonasal symptoms, including congestion-type symptoms. Interesting for the congestion thesis, but observational and not causal.
Link: https://pmc.ncbi.nlm.nih.gov/articles/PMC9335247/
CBD and Inflammatory Markers in Advanced Cancer — Randomized Trial
Year Published: 2023
Possible Indication: Systemic inflammation; cancer-related inflammation; safety
Key Takeaway: Trial measured inflammatory markers such as CRP in advanced cancer patients. It did not establish a clean broad anti-inflammatory clinical benefit. Useful because it shows that human biomarker evidence remains mixed.
Link: https://pmc.ncbi.nlm.nih.gov/articles/PMC10576726/
Antiviral Activity of Hemp Cannabinoids — Review
Year Published: 2023
Possible Indication: Antiviral; viral entry/replication; immune modulation
Key Takeaway: Summarizes antiviral signals from hemp cannabinoids, including possible effects on viral entry, replication, and immune response. Interesting, but still mostly preclinical and hypothesis-generating.
Link: https://pmc.ncbi.nlm.nih.gov/articles/PMC10133872/
Cannabis Smoke and Influenza A in Mice
Year Published: 2023
Possible Indication: Flu; respiratory safety; smoked-route risk
Key Takeaway: Important cautionary study. Cannabis smoke exposure disrupted host defense and increased viral burden in influenza-infected mice. This cuts against smoked cannabis as a sensible route during respiratory viral illness.
Link: https://pubmed.ncbi.nlm.nih.gov/38020563/
Cannabis Use and Chronic Rhinosinusitis Risk
Year Published: 2025
Possible Indication: Sinus symptoms; congestion; chronic rhinosinusitis
Key Takeaway: Retrospective observational study suggesting a possible relationship between cannabis use and lower chronic rhinosinusitis risk. Interesting sinonasal signal, but not proof that cannabis treats congestion or colds.
Link: https://pmc.ncbi.nlm.nih.gov/articles/PMC12658615/
FDA-Linked CBD Safety Trial — Liver Enzyme Elevations
Year Published: 2025
Possible Indication: Safety; liver risk; high-dose CBD
Key Takeaway: Randomized trial in healthy adults found that daily CBD at clinically meaningful doses caused liver enzyme elevations in some participants. Important safety caveat, especially for high-dose CBD or drug interactions.
Link: https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2836267
CBD/THC and Inflammatory Biomarkers — Systematic Review / Meta-Analysis
Year Published: 2025
Possible Indication: Systemic inflammation; cytokine response; biomarker evidence
Key Takeaway: Human evidence across inflammatory biomarkers remains mixed. Cleanest summary: cannabinoid anti-inflammatory biology is real, but human clinical evidence is not yet definitive.
Link: https://www.mdpi.com/1422-0067/26/23/11618